
Magic Salamanders & the Zero-Point Field (2 of 5)
Hallucinating for Health

In Part 1, we gave a basic overview of some key findings of Dr. Robert O. Becker’s research outlined in his book, “The Body Electric”. However, being that Becker utilized different equipment (DC vs. EEG) to measure changes in brain activity, we must provide a translation to what it refers to based on more commonly utilized neuroscience equipment.
The electroencephalogram (EEG) is a device that utilizes electrodes placed on the scalp to measure micro electric currents on the scalp of a person’s head. These micro electric currents have been associated with changes in perception. As we’ve outlined in past pieces, during non-dream sleep, the slowest wave (delta) dominates most of the activity. During normal, waking hours faster alpha and beta waves dominate most of the activity. However, being that dozens of electrodes are planted across the scalp, there is generally a variation of background activity taking place simultaneously in different areas.
Becker preferred the direct current (DC) measurement claiming that it generated a cleaner signal with less artifacts and the need to interpret multiple signals from multiple locations all at once. In terms of translating the DC signals to EEG for communicative purposes, Becker showcased that during normal waking consciousness, the direction of the DC current was observed to have a negative frontal potential and a positive posterior potential indicating an alpha/beta equivalent. By contrast, in deep sleep and anesthesia the direction of the DC current reverses to a positive frontal potential and a negative posterior potential indicating that this is equivalent to a delta dominant EEG.
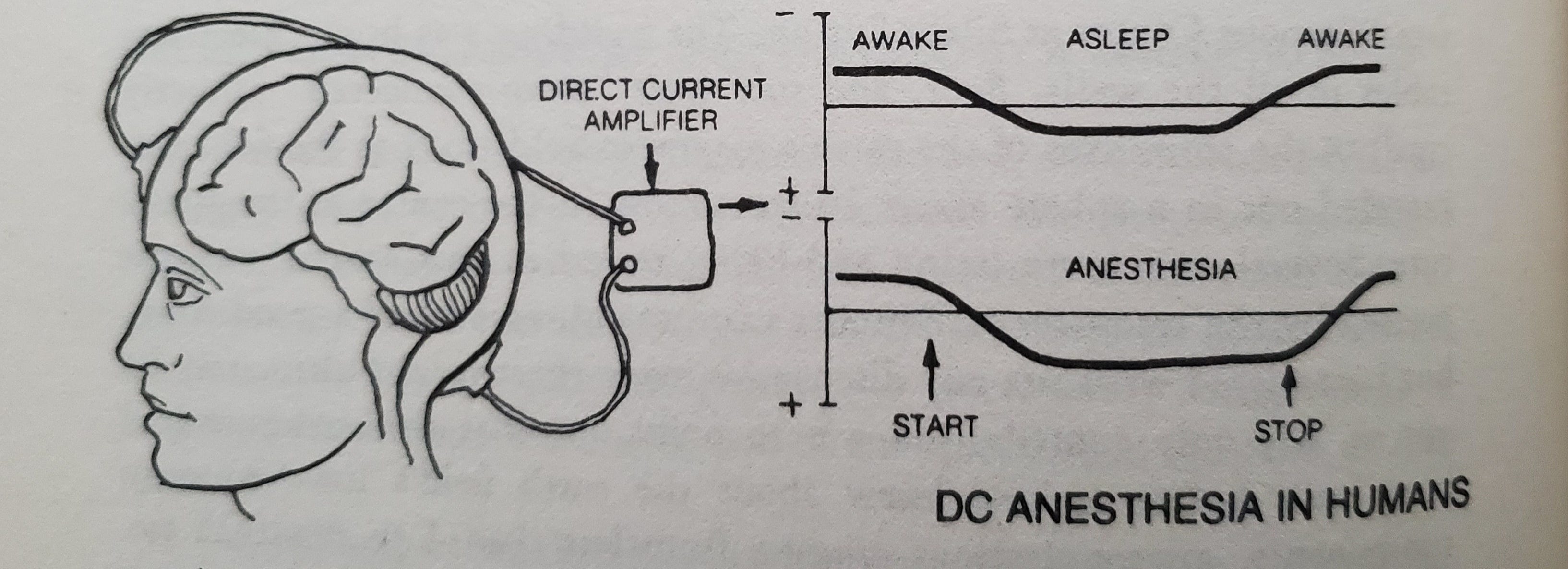
This all seems rather straightforward but the question is… what is the DC current equivalent when we see an increase in both slow waves (theta/delta) and fast waves (gamma) simultaneously as consistently seen during altered states of consciousness? The frontal potential cannot be both positive (slow wave) and negative (fast wave) at the same time. Based on the following excerpt from The Body Electric, it seems that instead of being a positive or negative frontal potential, the reading goes to zero: “In each case, I found that the frontal negative potential of the head became less negative, often reaching zero, as the client attained deep trance. The reading changed in the same direction as in anesthesia, only not as far.”
We interpret this finding as equal amplitude of opposite directional charges (theta and gamma) brings the brain’s electric field to zero when interpreted via DC measurements. According to Joachim Keppler’s model of consciousness based on the zero-point field (ZPF) and quantum electrodynamics (QED), the ZPF is unrelated to classic electric fields such as DC currents. However, electrically charged particles are related to the QED equation indicating that this change in neuroelectrophysiology could indicate an altered interplay with the ZPF. Being that the ZPF is proposed to contain all experiences and phenomenal qualities, we believe that cross-frequency coupling of slow and fast waves (EEG)/zero frontal potential (DC) indicate enhanced access to experience and information.
As we presented in a recent piece, we showcased evidence indicating that memories are likely to be stored in the ZPF rather than the physical brain. The ability to access the ZPF in a fluid manner depends on the neural oscillatory activity. There is evidence to suggest that theta-gamma coupling occurs during successful memory recall (Axmacher et al., 2010; Katerman et al., 2021; Solomon et al., 2017). When a subject is suffering from Alzheimer’s disease, they have an imbalance of theta-gamma coupling with a pronounced theta band and an impaired gamma band (Chen et al., 2023). This potentially indicates that imbalanced cross frequency coupling can impair fluid access to the ZPF leading to subpar memory recall.
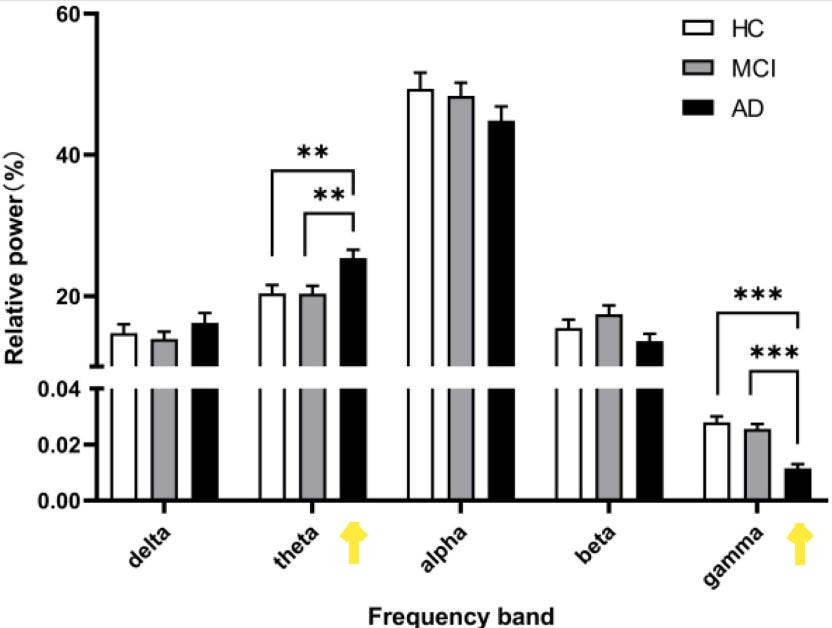
(Figure 2. from Chen et al., 2023, where you can see a distinct difference in the theta and gamma bandwidths in Alzheimer’s patients compared to healthy controls.)
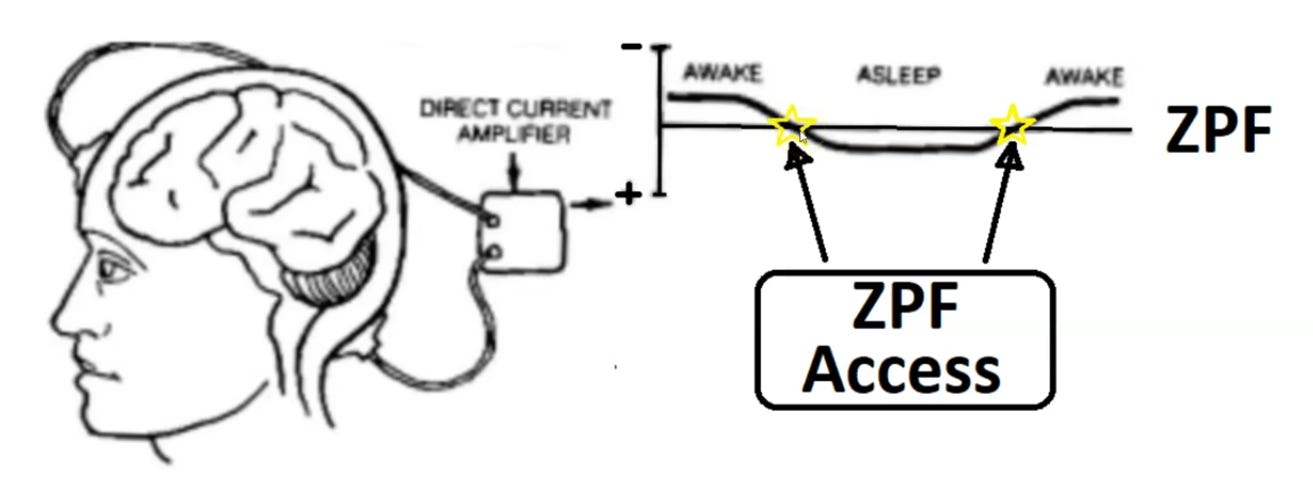
(An image of what we perceive to be a tighter coupling with the ZPF during states of consciousness in between being awake and asleep.)
It’s interesting that different equipment can offer a much different perspective of the same brain activity taking place. If all possibilities emerge from the ZPF, connecting with it in an amplified manner would seemingly afford more possibilities to occur… such as a person being able to get a large molar extracted from their mouths without feeling any discomfort. Based on Becker’s observation, this reading of the frontal potential reaching zero seems to coincide with enhanced possibilities based on intent/will.
When a local anesthetic such as procaine is administered to an injured limb, it induces a reversal of the baseline negative potential at the site of injury. However, this exogenous local anesthetic has no effect on the brain’s DC measurement. By contrast, hypnosis changes the brain’s DC measurement and when accompanied by a suggestion for pain control, the arm potential reversed in the same manner it does from a procaine injection and the pain signal is abolished.
What’s intriguing is that during hypnoanalgesia mediated surgery, the subject not only has control over the pain of the procedure but they also have shown distinct capabilities to alter blood coagulation of the wound. An example of this would be a dentist removing a wisdom tooth that leads to excessive bleeding at the wound site. The subject under hypnosis can be instructed to stop the bleeding immediately and the bleeding stops in an accelerated manner (Jones, 1951; Moss, 1957). The precision of the results of this instruction is fascinating as it doesn’t seem to be a systemic reaction of decreased blood flow or increased systemic coagulation. It is site specific, time specific, and noticeably effective. In the book “The Future of the Body” by Esalen co-founder Michael Murphy, he writes, “Several researchers, however, after long-term research with many subjects, have found that awareness can indeed develop around subtle feats of self-control such as a single nerve cell’s firing” (Green et al., 1969). This indicates the precision of one’s intent to influence specific activity of a very specific location in the body when the brain has a specific signature.
Theoretically speaking, the concept of formalized hypnosis might not be entirely necessary to induce this type of phenomena as long as a person is able to maintain a specific oscillatory signature in conjunction with sustained focus. We will touch up on this concept later on in this series.
Another interesting example of strange phenomena during hypnosis is the acceleration of wound healing. There are multiple points of evidence indicating that those that undergo hypnoanalgesia for surgery recovery significantly faster than subjects that utilize general or localized anesthesia (Ginandes et al., 2003).
A dramatic example of accelerated wound healing would be based on the work of a medical doctor based out of Louisiana named Dr. Dabney Ewin. This doctor worked in an emergency ward in that crazy city of New Orleans in the 1960’s and 70’s. He would regularly see patients arriving to the ward with second and third degree burns. Dr. Dabney observed that if he was able to treat the patients within a few hours of the initial burn, he could have great success in drastically speeding up the healing process. His protocol was based on utilizing a combination of hypnosis and encouraging the patient to hallucinate that they were cool and comfortable. If successful, the patient could experience a recovery period of 10 days compared to 90 days. However, if the patient was not seen within hours of the injury, the effects were much less pronounced (Ewin, 1983; Ewin, 1992). It’s entertaining to postulate that willfully inducing hallucinations via upregulation of hallucinatory molecules in the brain (DMT’s) are pertinent in this process.
(An interview of Dr. Ewin discussing his experience utilizing hypnosis & conscious hallucinations to accelerate healing for burn victims.)
An interesting phenomena that’s been observed consistently in the pediatric medical profession is the ability of young children to regenerate their severed fingers (Douglas, 1972; Illingworth, 1974). This occurs if the wound is merely kept clean and does not undergo any stitching. While many believe this is simply based on the proliferation of stem cells and growth hormone from growing children, there could be more to the story electrically speaking. As we cited in past pieces, young children exude EEG activity dominated by theta (Orekhava et al., 2006; Cellier et. al, 2021) and gamma frequencies (Takano et. al, 1998, Tiernay et. al, 2013). This brain activity essentially mimics that of a person under hypnosis. Unfortunately, we can only speculate on whether the DC frontal potential measurement of children is zero similar to that of adults under hypnosis. Whether this plays a role in autonomic regeneration of finger tips in children is unknown but there is a possibility that there is a connection.

(Figure 3., from Illingworth, 1974)

(Figure 1., from Douglas, 1972)
While autonomic regeneration in children is fascinating, our primary interest is the phenomena of altering the autonomic response based on intent/concentration in combination with altered states. As we know based on the excerpts from The Body Electric presented in Part 1, following injury or amputation of a limb, the negative potential of the site of injury quickly reverses to positive. This DC reversal also takes place in the head approximating the signal of delayed pain. This process then reverses significantly for the salamander in which the potential exceeds -30 mv compared to the lowly frog which continues with it’s slowly declining positive voltages. As we’ve cited in Part 1, the frontal potential of both human and salamander heads are negative when in normal waking consciousness and are even more negative during physical or mental activity. The direct current direction reverses during sleep and anesthesia which leads to the frontal potential to become positive. During hypnosis, Becker states that the normally negative positive potential becomes less negative and often reaches zero during deep trance. Following this trance, based on the suggestion given, the potential of the extremity or area of the focus can change accordingly. We must remember, based on EEG measurement deep trance occurs when slow wave amplitude increases (theta/delta) and the concentration/focus coincides with the fast wave (gamma) occurrence.

(An illustration showcasing the changes coinciding during salamander regeneration vs. sad frog non regeneration while overlaying the DC changes with the effects of hypnosis combined with concentration.)
The question that lingers is… is there any evidence that adult humans can utilize the combination of deep trance in combination with focused hallucinations to induce measurable changes to their physiology beyond pain control, blood coagulation, and accelerated wound healing?
Yup.
Stay tuned for Part 3!
PS. It seems as though negative frontal potential coincides with the linear perception and passage of time. If one were to look at the regenerative processes that take place during sleep coinciding with the positive frontal potential it’s almost akin to the body going reverse in time as it is attempting to retain a prior state of biology. However, during sleep, the DC reversals are systemic inducing systemic repair rather than targeted. During trance it seems that there can be targeted repair based on concentration and specific intent.